Diabetic Foot / Peripheral Vascular Disease / Peripheral Artery Disease
- Home
- Diabetic Foot/Peripheral Vascular Disease/Peripheral Artery Disease
A condition in which atherosclerotic plaque narrows or blocks arteries supplying blood to the limbs (usually legs), leading to reduced blood flow and ischemia.
When narrowing occurs in the heart it is called coronary artery disease while in the brain it is called cerebrovascular disease.
Peripheral artery disease most commonly affects the legs, but other arteries may also be involved. The affected blood vessels continue to narrow over months and years, and at some point the arteries become completely blocked.
MOSTLY AFFECTED ARTERIES:
- Sup femoral artery
- Popliteal artery
- Tibial/peroneal arteries
CLINICAL FEATURES:
A. SYMPTOMS:
- Intermittent claudication- The classic symptom is leg pain while walking which gets resolved with rest.
- Rest Pain- occurs at night which is relieved by hanging leg down.
- Non healing ulcers/gangrene-on toes or feet
- Up to 50% of cases are without symptoms.
B. SIGNS:
- Cold limb
- Poor nail and hair growth
- Thin, shiny skin
- Muscle wasting
- Reduced/ absent pulses
C. COMPLICATIONS:
- Critical limb ischemia.
- Poor wound healing.
- Infection or gangrene (tissue death) which may require amputation
- High cardiovascular risk (MI, stroke, death)
B. RISK FACTORS:
Non-modifiable
- Age >50
- Family history
- Genetic predisposition
Modifiable
- Smoking (most important)
- Diabetes mellitus
- Hypertension
- Dyslipidaemia (abnormal level of lipids in bloodstream).
- Obesity
- Sedentary lifestyle (lack of physical exercise)
- Chronic kidney disease
DIAGNOSIS:
A.CLINICAL EXAMINATION
Pulse examination- femoral a, popliteal a, dorsalis pedis a, post tibial a.
B. IMAGING
- Duplex doppler ultrasound → first-line
- CT angiography
- MR angiography
- Digital subtraction angiography (gold standard)- used before intervention.
MANAGEMENT/ TREATMENT PLAN:
There are three lines of treatment, based on the severity of the disease
A.Lifestyle Modification (for all patients)
- Smoking cessation
- Exercise therapy (supervised walking program)
- Weight reduction
- Control over Diabetes, Hypertension and lipids
- Foot care- Quick examination mnemonic:
- “CARE FEET”
- Check daily
- Avoid injury
- Right footwear
- Emollient for dry skin
- Foot hygiene
- Early medical help
- Exercise & stop smoking
- Trim nails straight
B.Medical treatment:
- Cholesterol lowering drugs like statins–reduce cardiovascular events.
- Drugs to counter hypertension.
- Antiplatelet drugs to prevent blood clots.
- Drugs for claudication
- Control comorbidities- ACE inhibitors, Strict glycemic control
C.Revascularization:
Revascularization aims to restore adequate blood flow to ischemic tissues in patients with significant symptoms, non-healing ulcers, or limb-threatening ischemia. It may be performed using endovascular techniques or open surgical procedures, depending on disease severity, anatomy, and patient factors.
Following are the methods
Angiography:
Angiography is an imaging procedure that uses contrast dye and X-ray guidance to visualize blood vessels and determine the exact location and severity of arterial blockages. It is essential for planning appropriate endovascular treatment.
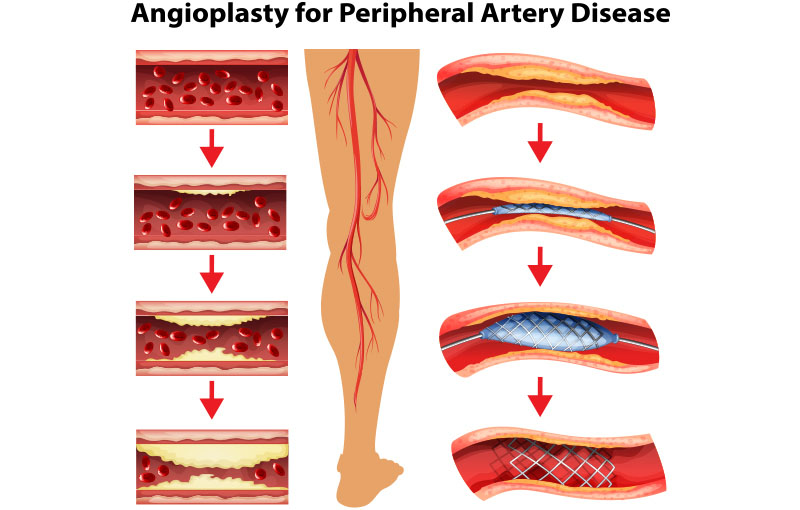
Angioplasty (including Drug-Eluting Balloons):
Angioplasty involves widening a narrowed artery using a balloon catheter to improve blood flow.
Drug-eluting balloons release antiproliferative medication at the treated site, which helps reduce restenosis and improves long-term vessel patency.
Stenting:
Stenting is the placement of a metal mesh scaffold inside the artery following angioplasty to keep the vessel open and maintain adequate circulation. Stents may be bare-metal or drug-eluting, selected based on lesion characteristics and risk of recurrence.
Atherectomy Devices:
Atherectomy uses specialized catheter-based devices to remove or debulk atherosclerotic plaque from the arterial wall. It is particularly useful in heavily calcified or resistant lesions where balloon angioplasty alone may not provide sufficient expansion.
Intravascular Lithotripsy (IVL) Balloon:
IVL balloons generate acoustic pressure waves within the artery to fracture deep calcium deposits, allowing better vessel expansion with low-pressure balloon inflation. This improves procedural safety and effectiveness in severely calcified peripheral arteries.
PREVENTION :
- Stop smoking
- Healthy diet
- Regular exercise
- Diabetes & Blood pressure control
- Lipid management
When to seek medical help?
- Contact a doctor immediately if you notice:
- Non-healing wound or ulcer
- Blackening of skin or toes
- Increasing redness, swelling, pus or fever
- Sudden severe foot pain or cold pale foot
- Loss of sensation
Case Study
Case - 1 :
45yrs male, heavy smoker and known diabetic for 7yrs had complains of severe leg cramps(Claudication) on walking for 100m. Angiography showed severe calcific stenotic occlusion at the left common iliac artery origin with a pressure gradient of >40mmHg. Also noted a plaque at the right common iliac artery causing 50-60% narrowing.
Bilateral common Iliac artery balloon mounted stent deployment done.
Post deployment, the left Iliac artery pressure gradient normalised.
Case - 2 :
62yrs female, with uncontrolled diabetes and also has hypertension on regular medication came with a non healing wound involving the left great toe. On examination, no peripheral pulses felt.
Angiography showed diffuse atherosclerotic changes involving the left leg arteries with a focal 3-4 cm severe calcific stenotic occlusion at the mid Superficial Femoral artery with sluggish flow in the leg.
Left superficial Femoral artery was stented and balloon angioplasty done.
Post angioplasty, all the peripheral pulses were felt. The wound healed in one month.
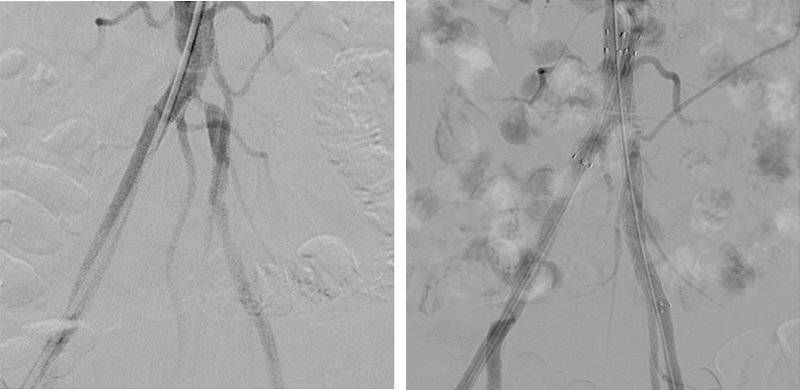
ILIAC ARTERY STENOSIS
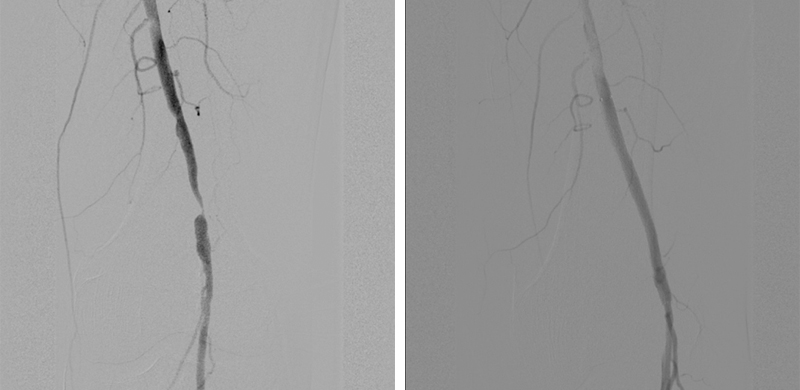
SUPERICAL FEMORAL ARTERY STENTING
Frequently Asked Questions?
Revascularization is recommended when blood flow to a limb is severely reduced, causing significant pain, non-healing wounds, or risk of limb loss. The goal is to restore circulation, relieve symptoms, and prevent complications.
Most endovascular procedures are minimally invasive and performed under local anaesthesia with mild sedation. Patients usually feel little to no pain during the procedure and only mild soreness afterward
The duration varies depending on the number and complexity of blockages, but most angiography-guided treatments take about 30 minutes to 2 hours
Many angioplasty or stenting procedures are short hospital stay procedures. Some patients may require overnight observation, especially if the disease is severe or multiple vessels are treated.
Recovery is usually quick. Most patients can walk within a few hours and resume normal daily activities within a few days, though strenuous activity may be restricted for about a week.
Yes, they are generally safe and minimally invasive. However, like all medical procedures, there are small risks such as bleeding at the puncture site, vessel injury, infection, allergic reaction to contrast dye, or re-narrowing of the artery.
Restenosis means the artery becomes narrow again after treatment. Drug-eluting balloons, stents, and proper medications help reduce this risk, but follow-up is important.
Yes. Patients usually need blood thinners, cholesterol-lowering drugs, and diabetes or blood pressure control to keep arteries open and prevent new blockages.
Peripheral artery disease is a chronic condition. Even after successful revascularization, lifestyle changes such as quitting smoking, healthy diet, exercise, and regular follow-up are essential to prevent recurrence.
Seek immediate care if there is severe pain, sudden swelling, bleeding from the puncture site, fever, loss of limb movement, or change in skin colour or temperature.